Tibial hemimelia – a rare congenital malformation whose treatment presents a serious challenge. The appropriate therapeutic approach varies depending on the many subtypes and associated deformities of the knee and ankle. Amputation is still considered the most widely accepted treatment, but it is generally not preferred by families. As a result, other reconstructive options have been developed. In the following two cases, we performed knee joint reconstruction by fusing the ankle joint, instead of amputation. This technique has not been described in the literature to date and has been named the Chabukoglu reconstructive technique or cruroplasty.
Introduction
Tibial deficiency (TD) is a congenital lower limb defect that can manifest through various abnormalities of the tibia, ranging from hypoplastic (underdeveloped) to complete absence of the tibia. The fibula is present and may be normal or dysplastic. This rare condition affects approximately one in a million live births in the United States. This phenomenon can be sporadic or associated with a family history. The anomaly can be unilateral or bilateral, appearing as an isolated deformity or as a symptom of a more complex malformation syndrome. Most commonly, one leg is observed to be shorter than the other. Knee and ankle abnormalities are common, as are cutaneous signs such as dimples above the head of the fibula or at the end of the tibia.
There are several classification systems for tibial hemimelia. The diagnosis is divided into four types, based on radiographic findings according to the 1978 Jones classification, which is often used in clinical practice. In 1985, Kalamchi and Dow refined it, and in 2008, Weber created an MRI-based classification. The newest system was formulated by Paley in 2003 and updated in 2016.
Treatment options for tibial hemimelia remain controversial. The gold standard for severe cases with complete absence of the tibia is a knee disarticulation followed by prosthetic fitting. Successful cases of early childhood amputation have been reported in the literature. Although families are often resistant, the functional outcomes of amputation, the most conventional treatment method, are remarkable. The treatment method varies depending on the presence of the proximal tibia, the presence of the patella, and the condition of the quadriceps mechanism.
In the present work, we present two cases of tibial hemimelia that do not fall into any of the existing classifications, along with a new surgical method that will open the way for alternative treatment options.
 Case 1
Case 1
An unrelated 3-year-old boy was admitted during an outpatient consultation eight years ago. Antenatal absence of the ipsilateral tibia and fibula was diagnosed during a routine ultrasound. There was no history of teratogenic drug use during the mother's pregnancy. The mother delivered the patient at 22 years of age via Cesarean section at 36 weeks gestation. The pregnancy was uneventful. No limb agenesis was observed in the family. The child had no other systemic anomalies besides tibia and fibula agenesis. Genetic analysis was not performed at the hospital where he was born. In examinations by other physicians, knee disarticulation and prosthetic ambulation were recommended.
During the initial examination, it was noted that the patient walked using their right foot and left knee due to the length discrepancy. While standing, they stood with their left foot fully planted (plantigrade), while the right foot did not touch the ground (Fig. 1 A, B).
Fig. 1. Image of the child's lower extremities during walking
Image of the child's lower limb in a standing position
The patient's standing posture is illustrated below as medical drawings (Fig. 2. A. B. C.). Furthermore, the absence of the fifth metatarsal on the same leg was noted.
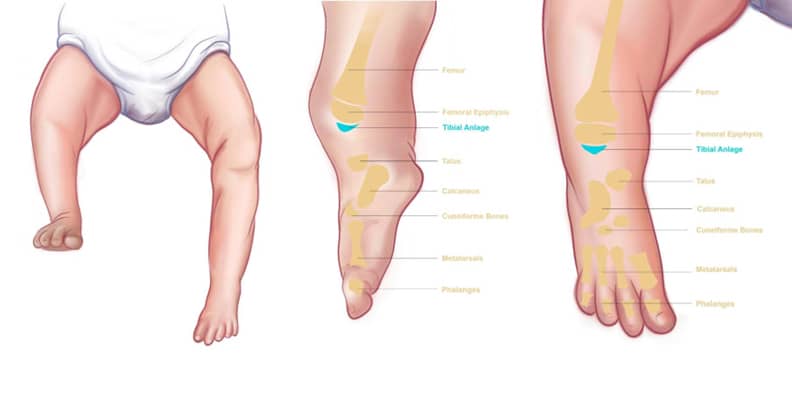
Fig. 2: A. Medical drawings of a child in a standing position
B. Lateral view
Anteroposterior view
The patient's X-rays showed complete absence of the tibia and fibula (Fig. 3 A, B).
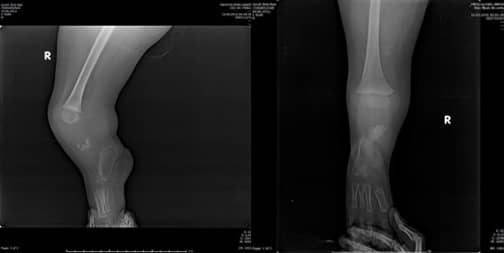
Fig. 3. A: Lateral view
Anteroposterior view
The patient underwent surgery at 3 years of age. Due to the presence of a tibial anlage and patellar tendon on magnetic resonance imaging (MRI), we decided to perform reconstructive surgery instead of a knee disarticulation. The preoperative view of the tibial anlage and ankle bones is shown in the picture (Fig. 2). One of the most important reasons for performing this surgery was to provide the child with a more functional gait. Therefore, we surgically removed the chondral parts of the calcaneus and talus and performed an arthrodesis (Fig. 4).

Fig. 4: Preoperative view showing the tibial remnant and talocalcaneal arthrodesis
Subsequently, after rotating the foot 90 degrees in the direction of plantarflexion (verticalization), we placed it under the tibial anlage and fixed the connection between the tibial anlage and the talocalcaneal ligament with Kirschner wires. The patient's lower limb was placed in a circular cast for two months postoperatively (Fig. 5).

Fig. 5: Postoperative view of the limb with a long leg cast
After the fusion of the talus with the tibial primordium, reconstructions of the collateral ligaments (LCL and MCL) were not performed, as it was unknown how the bone and cartilage would develop in a growing child. The toes were amputated to ensure proper prosthetic fitting and weight-bearing function.
Arthrodesis of the remaining bones in the mid and forefoot (metatarsals and tarsals) was not immediately considered, as the amputation stump would lengthen over time. We named this procedure „crus plasty“ and described it as the Chabukouchlou reconstruction technique.
Medical drawings and X-rays of this procedure are shown in Fig. 6. The ankle, which forms the crucis under the tibial primordium, can actively perform extension and flexion.
When the patient came to us for follow-up eight years later, it was found that they were experiencing pain due to a posterior-lateral tibial plateau osteophyte, as well as valgus deformity and a loss of approximately 25 degrees of knee extension.
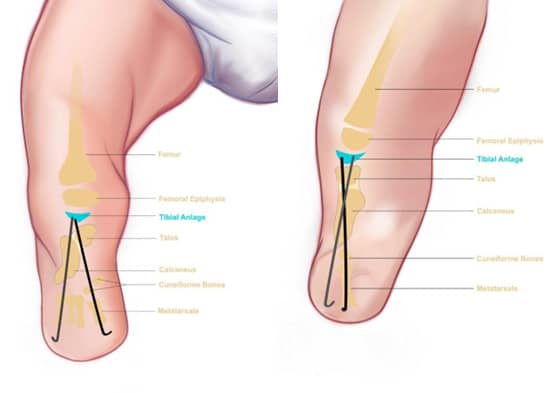

Fig. 6. A, B. Medical drawings of the Chabukoolu reconstructive technique
C, D. Postoperative X-rays
After the cast was removed after two months, the patient began to bear weight with the prosthesis, and knee movements started to take on load in the standing position with the prosthesis. Over time, it was observed that the bone thickness increased as a result of cartilage ossification and due to the load applied by the patient, in accordance with Wolff's law. Meanwhile, the patient underwent active physiotherapy. At the end of this process, quadriceps strengthening was performed. It was observed that the bones of the foot and ankle, which form the crus below the tibial primordium, could actively perform extension and flexion.
When the patient presented for follow-up eight years later, he was found to be experiencing pain due to a posterior-lateral osteophyte of the cruciate ligament, valgus deformity, and approximately 25 degrees of knee extension deficit (Fig. 7A, B).

Fig. 7: A: Sagittal view
Coronal view
The folding range was almost complete. As a result, surgery was recommended to correct the mechanical axis in order to achieve almost complete knee extension and to remove the bone spur that was pressing on the prosthesis. An open wedge osteotomy was planned to prevent shortening of the crus remnant, according to the patient's X-ray.
Preoperative imaging showing the valgus and flexion deformities of the affected leg (Fig. 8 A, B).

Fig. 8: Preoperative images showing
A. Genu valgum
25-degree flexion contracture
The operation was performed with preservation of the patellar tendon and removal of the cuneiform-metatarsal ligament, which was pressing on the skin. During the measurements, an open cuneiform osteotomy was performed to correct the deformity in two planes due to the presence of a bi-sagittal deformity. The removed cuneiform-metatarsal ligament was placed in the empty osteotomy zone for fusion, and fixation was achieved with a plate and screws (Fig. 9 A, B, C, D, E, F).

Fig. 9
Open wedge osteotomy
The author's foot graft from the 4th metatarsal was removed.
Plate and screw fixation
Postoperative anteroposterior view
E: Postoperative lateral view
Postoperative hair view
At the end of the second postoperative month, the patient had no pain, and radiography showed bone union at the osteotomy site (Fig. 10 A, B).

Fig. 10. After 2 months, the X-ray shows bone fusion of:
A. Lateral view
A. Anteroposterior view
Case 2
A 7-month-old boy was referred to our clinic due to severe deformation of his left foot. Absence of the 5th ray of the right foot, a defect of three rows, and talipes equinovarus deformity of the left foot were diagnosed (Fig. 11 A, B). Family history was negative for limb anomalies. The patient had a normal quadriceps tendon and patella.


Fig. 11. A. Clinical images of the affected side
B. X-rays of the affected side
The patient's sister has no limb abnormalities. The mother delivered via C-section at 38 weeks gestation at the age of 23. The mother's pregnancy was uncomplicated. There is no history of teratogenic medication use during pregnancy. The mother did not have any febrile illnesses during this period. The patient has not undergone genetic testing.
The Chabutkoo reconstructive technique was also applied to this patient. An arthrodesis between the talus and calcaneus was performed, as in the previous case. Additionally, no arthrodeses of the midfoot and forefoot joints were performed to prevent growth arrest of the bones. Subsequently, an arthrodesis between the tibial anlage and the talus was achieved, fixed with two Kirschner wires, and the patellar tendon was sutured to the talus. The toes of this patient were also amputated to adapt the prosthesis to the residual limb.
During the pediatric follow-up, no surgical intervention was performed on the right side. The flexion range in the left knee was assessed at 50 degrees. This child actively used a below-the-knee prosthesis and had no complaints (Fig. 12 A, B).
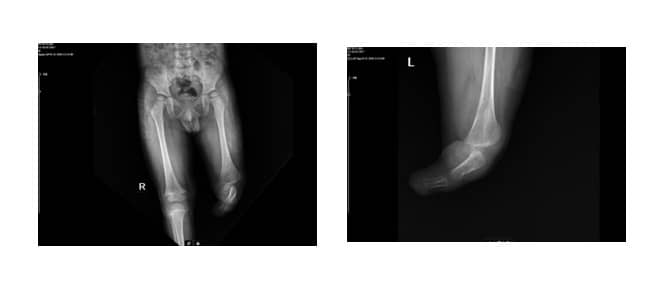
Fig. 12. X-rays 2 years after surgery
A. Anteroposterior X-ray
V. Lateral X-ray
Discussion
Several classification systems for tibial hemimelia (TH) have been proposed. Jones published his first classification in 1978, based on radiographic findings. Thirty years later, Weber introduced a new classification system that considers both radiographic data and the cartilaginous anlage. Paley found that when using his classification system, no unclassifiable cases were identified. However, these two cases do not fall into any of the three classification systems.
Actually, our goal in this case series was to create a functional knee using the available foot and ankle, and to convert a knee disarticulation to a more functional below-knee amputation. In these two cases, reconstruction was performed rather than amputation, due to various reasons.
First, amputation is not an accepted form of treatment in our culture, as it was in Egyptian and Persian cultures. Authors often encounter older children and teenagers with various congenital limb defects who use crutches and walk on their knees, but nevertheless refuse to undergo amputation of one of their limbs.
Second, the presence of the quadriceps tendon and patella in the knee joint prioritizes reconstruction over disarticulation. Based on the fact that both patients had a patella and quadriceps, we performed reconstruction using the Chabucoolu technique.
One of the reasons for choosing knee reconstruction over knee disarticulation was to create a more active leg by preserving the existing bones and joints, along with the proprioceptive and sensory function of the foot.
The presence of a tibial bud guided us towards reconstruction instead of amputation.
Actually, in some cases of tibial hemimelia, we mimicked the ankle structure by fusing the calcaneus and talus.
In severe forms of tibial hemimelia, as in our cases, the dysplastic calf muscles and distal femoral condyles are insufficient to cover the disarticulated residual limb in patients. Therefore, if disarticulation is performed, skin complications such as wound dehiscence, ulcer development, and calluses may arise due to pressure concentration on the small weight-bearing residual limb and the lack of adequate soft tissue coverage. These problems prolong hospital stays and hinder early and active prosthetic rehabilitation.
Previous research
Previous studies have shown that the distal femoral epiphysis accounts for more than two-thirds of bone growth. Therefore, the outcome may be the same as with amputation in the middle of the femur. Normal femoral growth is not affected by knee disarticulation or other palliative procedures.
According to Brown, centralization of the fibula offers the patient the advantages of a below-knee amputation, with the patient functioning better than with an above-knee amputation. A study by Behr and colleagues found that patients with below-knee amputations had a better history of prosthetic use, better prosthetic fit, less energy expenditure during ambulation, and faster walking speeds in adverse weather conditions compared to other amputation levels.
Literature
- Fang WH, Thomas E, Fan J, Leis AR, Rosenfeld SR. Bilateral calcaneal transfers for congenital tibia deficiency: a novel surgical technique and case report. JAAOS Global Research & Reviews. 2022;6(12). doi:10.5435/JAAOSGLOBAL-D-22-00070
- Weber M. New classification and assessment for tibial hemimelia. J Child Orthop. 2008;2(3):169. doi:10.1007/s11832-008-0081-5
- Basso M, Camurri V, Frediani P, Boero S. A rare case of tibial hemimelia, surgical technique, and clinical outcome. Acta Orthop Traumatol Turc. 2018;52(4):315-319. doi:10.1016/J.AOTT.2017.11.004
- Pattinson RC, Fixsen JA. Management and outcome of tibial dysplasia. J Bone Joint Surg Br. 1992;74(6):893-896. doi:10.1302/0301-620X.74B6.1447253
- Paley D. Tibial hemimelia: a new classification and reconstructive options. J Child Orthop. 2016;10(6):529. doi:10.1007/S11832-016-0785-X
- Matsuyama J, Mabuchi A, Zhang J, et al. Siblings with bilateral tibial hemimelia born to phenotypically normal parents. J Hum Genet. 2003;48(4):173-176. doi:10.1007/S10038-003-0003-9
- Gollop TR, Lucchesi E, Martins RMM, Nione AS. Familial occurrence of split femur and monodactylous ectrodactyly. Am J Med Genet. 1980;7(3):319-322. doi:10.1002/AJMG.1320070313
- Chong DY, Paley D. Surgical Reconstruction of Tibial Hemimelia Deformities. Children (Basel). 2021;8(6). doi:10.3390/CHILDREN8060461
- Jones D, Barnes J, Lloyd-Roberts GC. Congenital aplasia and dysplasia of the tibia with intact fibula. Classification and treatment. J Bone Joint Surg Br.
- 10. Kalamchi A, Dawe R V. Congenital Deficiency of the Tibia. J Bone Joint Surg Br. 1985;6(1):117. doi:10.1097/01241398-198601000-00038
- Weber M. A new classification and assessment for tibial hemimelia. J Child Orthop. 2008;2(3):169-175. doi:10.1007/S11832-008-0081-5
- Paley D. Tibial hemimelia: a new classification and reconstructive options. J Child Orthop. 2016;10(6):529. doi:10.1007/S11832-016-0785-X
- Shahcheraghi GH, Javid M. Functional assessment in tibial hemimelia (Is it possible to save the foot during reconstruction?). J Pediatr Orthop. 2016;36(6):572-581. doi:10.1097/BPO.0000000000000513
- Balci HI, Saglam Y, Bilgili F, Sen C, Kocaoglu M, Eralp L. Preliminary report on amputation versus reconstruction in the treatment of tibial hemimelia. Acta Orthop Traumatol Turc. 2015;49(6):627-633. doi:10.3944/AOTT.2015.15.0005
- Failure of fibular centralization in congenital tibial length deficiency – PubMed. Accessed July 30, 2023. https://pubmed.ncbi.nlm.nih.gov/2071619/
- Fernandez-Palazzi F, Bendahan J, Rivas S. Congenital deficiency of the tibia: a report of 22 cases. J Pediatr Orthop B. 1998;7(4):298-302. doi:10.1097/01202412-199810000-00008
- Farr S, Ganger R, Grill F. [Congenital tibial hemimelia]. Orthopade. 2014;43(11):1016-1021. doi:10.1007/S00132-014-3017-4
- Hosny GA. Treatment of tibial hemimelia without amputation: a preliminary report. J Pediatr Orthop B. 2005;14(4):250-255. doi:10.1097/01202412-200507000-00003
- Christini D, Levy EJ, Facanha FAM, Kumar SJ. Fibular transposition for congenital absence of the tibia. J Pediatr Orthop. 1993;13(3):378-381. doi:10.1097/01241398-199305000-00020
- Frost HM. The bone mechanostat: a 2003 update. Anatomical Record – Part A Discoveries in Molecular, Cellular, and Evolutionary Biology. 2003;275(2):1081-1101. doi:10.1002/ar.a.10119
- The Art of Limb Alignment [3rd ed.] – DOKUMEN.PUB. Accessed August 15, 2023. https://dokumen.pub/the-art-of-limb-alignment-3nbsped.html
- Jones D, Barnes J, Lloyd-Roberts GC. Congenital aplasia and dysplasia of the tibia with intact fibula. Classification and management. J Bone Joint Surg Br. 1978;60(1):31-39. doi:10.1302/0301-620X.60B1.627576
- Weber M. New classification and assessment for tibial hemimelia. J Child Orthop. 2008;2(3):169-175. doi:10.1007/S11832-008-0081-5/ASSET/IMAGES/LARGE/10.1007_S11832-008-0081-5-FIG7.JPEG
- Basso M, Camurri V, Frediani P, Boero S. A rare case of tibial hemimelia, surgical method, and clinical results. Acta Orthop Traumatol Turc. 2018;52:315-319. doi:10.1016/j.aott.2017.11.004
- Jayakumar SS, Eilert RE. Fibular transplant for congenital absence of the tibia. http://journals.lww.com/clinorthop
- Hootnick DR, Packard DS, Levinsohn EM, Cady RB. Soft tissue anomalies in a patient with congenital tibia aplasia and talocalcaneal synchondrosis. Teratology. 1987;36(2):153-162. doi:10.1002/TERA.1420360202
- Chinnakkannan S, Das RR, Rughmini K, Ahmed S. A case of bilateral tibial hemimelia type VIIa. Indian J Hum Genet. 2013;19(1):108-110. doi:10.4103/0971-6866.112924
- Lloyd S, Rashid AHA, Das S, Ibrahim S. Trans-tibial amputation in a patient with proximal femoral focal deficiency and tibial hemimelia: surgical anatomy and clinical implications. Anat Sci Int. 2014;89(2):122-125. doi:10.1007/S12565-013-0211-0
- Fujii H, Doi K, Baliarsing AS. Transtibial amputation with plantar flap for congenital deficiency of the tibia. Clin Orthop Relat Res. 2002;403(403):186-190. doi:10.1097/00003086-200210000-00027
- Sulamaa M, Ryöppy S. Congenital absence of the tibia. http://dx.doi.org/103109/17453676408989329. 2009;34(4):337-348. doi:10.3109/17453676408989329
- Sepúlveda M, Téllez C, Villablanca V, Birrer E. Distal femoral fractures in children. EFORT Open Rev. 2022;7(4):264. doi:10.1530/EOR-21-0110
- BROWN FW. Construction of the knee joint in congenital complete absence of the tibia (paraxial hemimelia of the tibia). Preliminary report. 1965. http://journals.lww.com/jbjsjournal
- Behr J, Friedly J, Molton I, Morgenroth D, Jensen MP, Smith DG. Pain and the impact of pain in adults with lower-limb amputation: comparison of knee disarticulation, transtibial, and transfemoral amputation levels. J Rehabil Res Dev. 2009;46(7):963-972. doi:10.1682/JRRD.2008.07.0085

